
Fact Check: "Catholic hospitals treat pregnancy complications without ever having to performing abortions"


🔺️ Content Warning: This article contains graphic descriptions of pregnancy loss and may be disturbing or triggering for some readers.
Outline:
Claim: Catholic hospitals treat pregnancy complications without ever having to performing abortions
The United States Conference of Catholic Bishops, the Catholic Health Care Leadership Alliance, the Christ Medicus Foundation, the National Catholic Bioethics Center, the Catholic Bar Association, the Catholic Medical Association, and the Catholic Benefits Association have submitted a joint brief of amici curiae urging the Supreme Court of the United States to effectively nullify federal protections for the health and lives of pregnant patients who require emergency abortions to prevent disability and death - guaranteed to patients by the Emergency Medical Treatment and Active Labor Act (EMTALA). The Supreme Court will hear oral arguments in the consolidated cases Idaho v. United States and Moyle v. United States next week.
In the brief, the Catholic groups (the Amici) contend that Catholic healthcare providers “have a consistent record” of stabilizing pregnant patients experiencing obstetric emergencies in compliance with (1) the Emergency Medical Treatment and Active Labor Act, (2) the Catholic Church’s Ethical and Religious Directives for Catholic Health Care Services (ERDs), (3) the Catholic Church’s moral teachings, and (4) medical ethics — without ever having to perform “direct abortions.” The intended implication is that no harm will come to pregnant patients should the Supreme Court nullify EMTALA's federal protections.
The Amici’s contention, however, is demonstrably, perniciously false.
Verdict: False ❌️
As I noted in the last newsletter, Catholic hospitals “have a consistent record” of violating EMTALA and dangerously “denying care to patients who are in the midst of a miscarriage or experiencing other pregnancy complications prior to viability—and who face increased risks with each passing” moment.1
Catholic hospitals must adhere to “a set of policy prescriptions known as the Ethical and Religious Directives for Catholic Health Care Services (‘the Directives’), which are issued by the United States Conference of Catholic Bishops (USCCB).”2 This means that pregnant patients “receive reproductive health care dictated by bishops rather than medical doctors,”3 with religious dogma carrying more weight than medical standards and ethics.4
“The directives state that abortion is never permitted.”5 Furthermore, the directives state that “the free and informed health care decision of the [patient]. . . is to be followed so long as it does not contradict Catholic principles.”6
“There is variation in how Catholic hospitals implement the Directives. Nevertheless... many Catholic hospitals comply with the Directives by prohibiting their physicians from performing an abortion or sterilization even when this denial of care puts a patient at serious risk, and others will deviate from the Directives only after the patient has already been harmed. Moreover, deviation can sometimes carry penalties—including the loss of the hospital’s ‘Catholic’ status—even when the hospital acts to save a woman’s life.”7
“The only treatment for a uterine infection, and some other pregnancy complications… is an abortion.”8 And “the longer the provider waits, the greater the risk that the infection could spread and the patient could become septic and need ICU-level care. That’s why… [doctors] intervene well before the patients’ lives are in danger. But at Catholic hospitals, policies don’t allow providers to act till the threat to the woman’s life is more immediate.”9
As documented below, physicians working in Catholic-owned hospitals across the United States are often “barred from completing emergency uterine evacuation while fetal heart tones [are] present, even when medically indicated.”10 As a result, hospitals have forced physicians “to delay care or transfer patients to non–Catholic-owned facilities.”11 In other instances, physicians choose to covertly defy Catholic authority and violate the protocol of their hospitals’ ethics committees, taking matters into their own hands in order to provide pregnant patients necessary standard of care.12
While Catholic authorities will often insist that Catholic hospitals value maternal and fetal life equally,13 Catholic doctrine effectuated necessarily establishes a value hierarchy in which fetal life is given supremacy,14 putting pregnant patients’ lives and health in jeopardy.
The following documented cases are illustrative.
Documented cases
Denials of care
🟥 Dr S, a perinatologist, was working at a Catholic hospital. Dr S recalled a case in which the refusal of the Catholic hospital’s ethics committee to approve a uterine evacuation (abortion) “not only caused significant harm to the patient but [also] compelled” Dr S to violate hospital protocol.15 The patient was only 19 weeks pregnant (LMP), and the pregnancy tissue was already protruding into her vagina. Because the patient’s pregnancy was not promptly terminated, the patient became septic and progressed into septic shock.
Note: In the quote below, Dr S refers to bleeding caused by stage 2 disseminated intravascular coagulopathy (DIC), as well as to vasopressors (“pressors”). To appreciate how incredibly ill Dr S’s patient was, it is important to first understand these terms: One byproduct of severe sepsis and septic shock is disseminated intravascular coagulopathy (DIC), a “serious condition that causes abnormal blood clotting throughout the body’s blood vessels.”16 DIC has two stages. “In stage one, overactive clotting leads to blood clots throughout the blood vessels. The clots can reduce or block blood flow, which can damage organs.”17 “In stage two, as DIC progresses, the overactive clotting uses up platelets and clotting factors that help the blood to clot. Without these platelet and clotting factors, DIC leads to bleeding just beneath the skin, in the nose or mouth, or deep inside the body.”18
Sepsis also causes toxins produced by bacteria to “damage the small blood vessels, causing them to leak fluid into the surrounding tissues.”19 This causes a patient’s blood pressure to drop and affects the heart's ability to pump blood to the body’s vital organs.20 When blood doesn't reach vital organs, such as the brain and liver, these organs are deprived of oxygen and begin to shut down.21 When this occurs, doctors will give a patient vasopressors (“pressors”), drugs used to make blood vessels constrict or become narrow, in an attempt to raise the patient’s blood pressure and prevent cardiac arrest.
Dr S recalled:
“I'll never forget this; it was awful— …she's septic to the point that I'm pushing pressors on labor and delivery trying to keep her blood pressure up, and I have her on a cooling blanket because she's 106 degrees. And I needed to get everything out [of her uterus]. And so I put the ultrasound machine on and there was still a [fetal] heartbeat, and [the ethics committee] wouldn't let me [evacuate her uterus] because there was still a heartbeat. This woman is dying before our eyes. I went in to examine her, and I was able to find the umbilical cord through the membranes and just snapped the umbilical cord… so that I could put the ultrasound— ‘Oh look. No heartbeat. Let's go.’ She was so sick she was in the [intensive care unit] for about 10 days and very nearly died… She was in DIC [disseminated intravascular coagulopathy]… Her bleeding was so bad that the sclera, the white of her eyes, were red, filled with blood… And I said, ‘I just can't do this. I can't put myself behind this. This is not worth it to me.’ That's why I left.”22
“From Dr S's perspective, the chances for fetal life were nonexistent given the septic maternal environment. For the ethics committee, however, the present yet waning fetal heart tones were evidence of fetal life that precluded intervention. Rather than struggle longer to convince his committee to make an exception and grant approval for termination of pregnancy, Dr S chose to covertly sever the patient's umbilical cord so that the fetal heartbeat would cease and evacuation of the uterus could ‘legitimately’ proceed.”23 Horrified by the Catholic hospital’s ethics committee, Dr S resigned.
In taking matter into his own hands, Dr S saved the patient’s life.
Savita Halappanavar, a 31 year old dentist expecting her first baby, was not so lucky. She died of septic shock at a Catholic hospital in 2012. The government report on her death details Savita’s demise. She, too, had developed DIC which caused blood clots to form in her lungs, and she was being given high doses of vasopressors as her heart rate continued to drop.24 “The patient suffered a cardiac arrest at 00:45 hrs on the 28th of October, 2012. Cardiopulmonary resuscitation was continued to 01:09 hrs. The patient was pronounced dead at 01:09 hrs.”25 Such unnecessary, preventable finality.
🟥 Dr H worked at a Catholic-owned hospital in the Midwest. Her patient was 14 weeks pregnant (LMP) and experiencing early pregnancy loss (EPL). When doctor H examined the patient, she observed a hand protruding through the patient’s cervix and into her vagina. The patient’s membranes had ruptured putting her at high risk of infection— risk that increased as each moment passed.
The Catholic-owned hospital’s ethics committee refused to approve a termination, because fetal heart tones could still be detected. Dr H “sent her patient by ambulance 90 miles to the nearest institution” so that her patient could receive necessary healthcare.26 Transporting the patient “was quicker and safer than waiting for the fetal heartbeat to stop while trying to stave off infection.”27 Dr H recalled:
“She was very early, 14 weeks. She came in … and there was a hand sticking out of the cervix. Clearly the membranes had ruptured and she was trying to deliver… There was a [fetal] heart rate, and [we called] the ethics committee, and they [said], ‘Nope, can't do anything.’ So we had to send her to [the university hospital]… Even if mom is very sick, you know, potentially life threatening, [we] can't do anything.”28
🟥 A doctor at a secular hospital in New England recalled a patient “who had previously been evaluated at a local Catholic hospital after she started bleeding around 12 weeks into her pregnancy. The Catholic hospital performed an ultrasound and found that the patient had an abnormal pregnancy ‘with placenta coming out of her cervix,’ but because there was a fetal heartbeat, they told her she would have to wait. When the patient presented at this doctor’s [secular] hospital a week later, she was hemorrhaging and severely anemic from her blood loss over the past week. The medical team at the secular hospital performed emergency surgery and was just barely able to avoid the need for a hysterectomy—but the patient had to stay in the intensive care unit and needed transfusion of seven units of blood during her hospital stay. None of this would have been necessary had the Catholic hospital provided appropriate care when the patient first presented.”29
Delays in Care
🟧 “Dr. David Eisenberg recalled that ‘the sickest patient I ever cared for during my residency’ was a young woman denied care at a Catholic hospital outside of Chicago, Illinois. Her water had broken well before the fetus was viable, but the hospital refused to take steps to hasten delivery even though everyone knew the fetus could never survive. By the time she was transferred to Dr. Eisenberg’s hospital 10 days later, she had a fever of 106 degrees and was dying of sepsis. She survived, but she suffered an acute kidney injury requiring dialysis and a cognitive injury due to the severity of her sepsis. She spent nearly two weeks in the hospital before being transferred to a long-term care facility.”30 Dr. Eisenberg recollected:
“I clearly remember sitting in her ICU room after her [uterine] evacuation, wondering if she would make it through the night… To this day, I have never seen someone so sick—because we would never wait that long before evacuating the uterus. Expediting the delivery is the right thing to do in such situations, always, regardless of the religious affiliation of the hospital.”31
🟧 “Dr. Rupa Natarajan was working in a Catholic hospital in New England when she encountered a 19-year-old pregnant woman experiencing preterm premature rupture of membranes at 17 weeks. The pregnancy was doomed, and the patient was getting very sick, so Dr. Natarajan determined that the best course would be to perform an abortion. But the hospital prohibited her from doing so. The patient was admitted but not treated, and over the next day, her temperature and heart rate climbed. By the time Dr. Natarajan could arrange to have her transferred to another hospital to save her life, the patient’s fever had reached 104 degrees.”32
🟧 Dr G was working at a southern Catholic hospital. Her patient was 14 weeks pregnant (LMP), and the patient’s membranes had protruded into her vagina. Dr G made the decision to circumvent the hospital’s ethics committee. “She opted not to check fetal heart tones or seek ethics committee approval when caring for a miscarrying woman for fear that documentation of fetal heart tones would have caused unnecessary delays.”33
“She was 14 weeks and the membranes were literally out of the cervix and hanging in the vagina. And so with her I could just take care of it in the [emergency room] but her cervix wasn't open enough … so we went to the operating room and the nurse kept asking me, ‘Was there heart tones, was there heart tones?’ I said ‘I don't know. I don't know.’ Which I kind of knew there would be. But she said, ‘Well, did you check?’ … I said, ‘I don't need an ultrasound to tell me that it's inevitable … you can just put, “The heart tones weren't documented,” and then they can interpret that however they want to interpret that.’ … I said, ‘Throw it back at me … I'm not going to order an ultrasound. It's silly.’ Because then that's the thing; it would have muddied the water in this case.”34
"Dr G's main concern was sparing the patient extended suffering during loss of pregnancy. She disregarded the authority and protocol of the hospital ethics committee by not checking for fetal heart tones, which, she believed, would have led to significant delay in the inevitable treatment.”35 “[A]ny delay that might be added to a procedure that is inevitably going to happen places that person at risk of serious, life-threatening complications,” including sepsis and organ infection.”36
🟧 After seeing a fetal limb in her toilet, a woman sought care at a Catholic hospital in Michigan. Staff dilated her cervix, causing “a bulging bag of waters” to protrude into her vagina.37 The hospital refused the patient’s request to break her water and begin pre-viability delivery.38 “The patient was forced to wait over eighteen hours, while dilated, to complete the miscarriage naturally, resulting in retention of the placenta (a leading cause of maternal hemorrhaging and death) and additional, and potentially unnecessary, surgical intervention to remove it.”39 A test of the placenta later showed that is was positive for infection.40
Patient dumping
🟨 “Dr B, an obstetrician–gynecologist working in an academic medical center, described how a Catholic-owned hospital in her western urban area asked her to accept a patient who was already septic. When she received the request, she recommended that the physician from the Catholic-owned hospital perform a uterine aspiration there and not further risk the health of the woman by delaying her care with the transport.”41
“Because the fetus was still alive, they wouldn't intervene. And she was hemorrhaging, and they called me and wanted to transport her, and I said, ‘It sounds like she's unstable, and it sounds like you need to take care of her there.’ And I was on a recorded line, I reported them as an EMTALA [Emergency Medical Treatment and Active Labor Act] violation. And the physician [said], ‘This isn't something that we can take care of.’ And I [said], ‘Well, if I don't accept her, what are you going to do with her?’ [He answered], ‘We'll put her on a floor [i.e., admit her to a bed in the hospital instead of keeping her in the emergency room]; we'll transfuse her as much as we can, and we'll just wait till the fetus dies.’”42
“Ultimately, Dr B chose to accept the patient to spare her unnecessary suffering and harm, but she saw this case as a form of ‘patient dumping,’ because the patient was denied treatment and transported while unstable.”43
Reach and influence
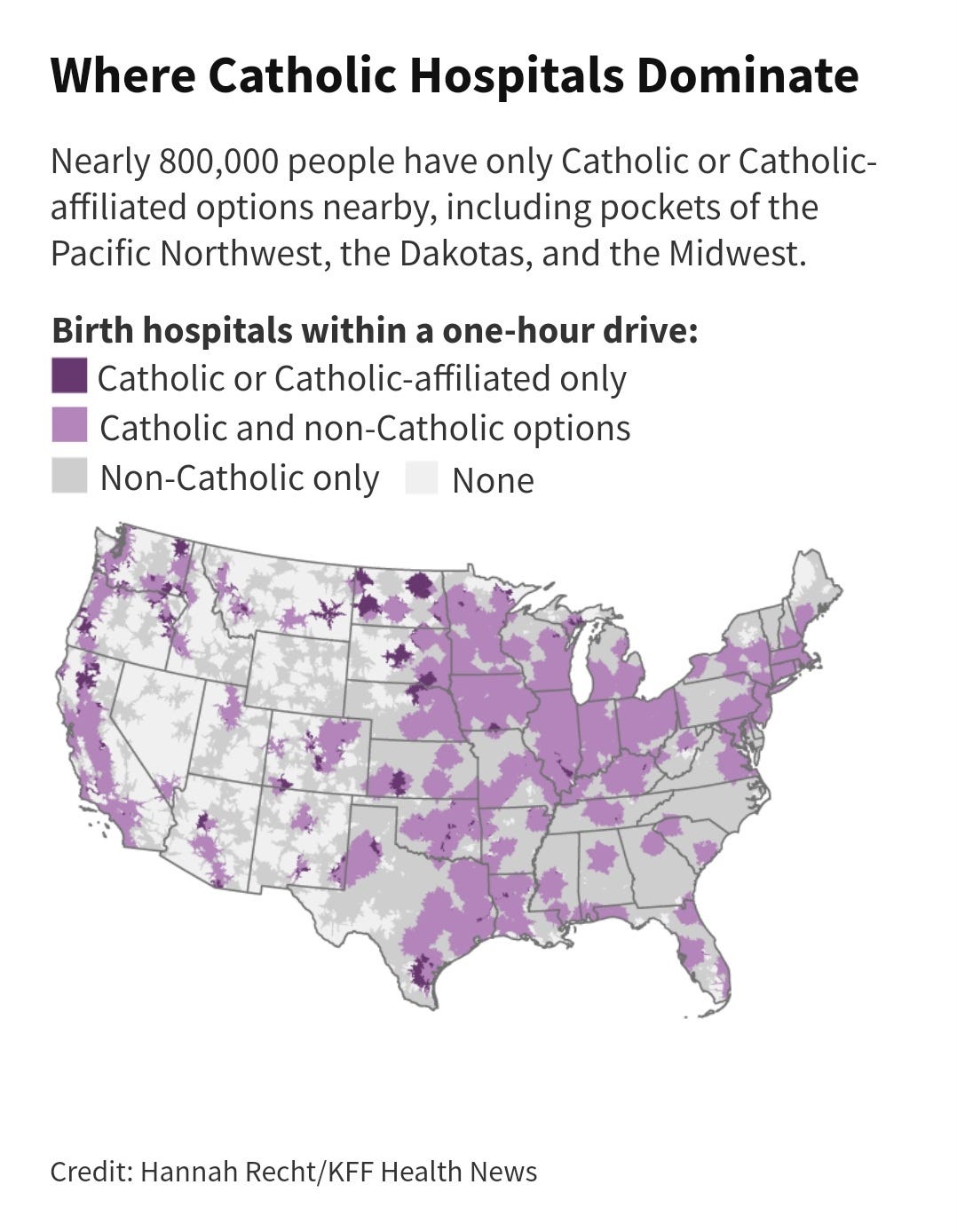
“More and more women are running into barriers to obtaining care as Catholic health systems have aggressively acquired secular hospitals in much of the country. Four of the 10 largest U.S. hospital chains by number of beds are Catholic, according to federal data from the Agency for Healthcare Research and Quality. There are just over 600 Catholic general hospitals nationally and roughly 100 more managed by Catholic chains that place some religious limits on care.”44
“Leaders in Catholic-based health systems have hammered home the importance of the church’s directives, which are issued by the U.S. Conference of Catholic Bishops, all men, and were first drafted in 1948. The essential view on abortion is as it was in 1948. The last revision, in 2018, added several directives addressing Catholic health institution acquisitions or mergers with non-Catholic ones, including that ‘whatever comes under control of the Catholic institution — whether by acquisition, governance, or management — must be operated in full accord with the moral teaching of the Catholic Church.’”45
A 2018 report, “Bearing Faith: The Limits of Catholic Health Care for Women of Color,” found that women of color are “more likely than white women to give birth at a Catholic hospital. In nineteen of thirty-three states and one territory, Catholic hospitals reported a higher percentage of births to women of color than did non-Catholic hospitals.”46 *Importantly, “these results indicate that pregnant women of color are more likely than their white counterparts to receive reproductive health care dictated by bishops rather than medical doctors.”47 “These results are especially troubling given that women of color already face numerous health disparities, including disproportionately high rates of maternal and infant mortality, which increases their need to receive reproductive health care that meets the highest professional standards.”48 The report’s findings also “indicate that women of color are at greater risk of being denied care due to religious restrictions when they need it most—during childbirth.”49
Black women already “face greater barriers to health care across a wide range of services” due to a number of factors, “including economic inequality and structural discrimination, which often work in tandem.”50
The report presents “some startling data. For example, in New Jersey, women of color make up half of all women of reproductive age but 80 percent of births at Catholic hospitals. And in Maryland, black women had almost 3,000 more births at Catholic hospitals than white women, despite the fact that they had over 10,000 fewer births overall. In 19 of 33 states and one territory, Catholic hospitals reported a higher percentage of births to women of color than did non-Catholic hospitals.”51 *An analysis conducted by ProPublica “showed how women who deliver at hospitals predominantly serving black women are at higher risk of harm. The impact of Catholic ethics restrictions on women of color should be examined alongside these trends.”52
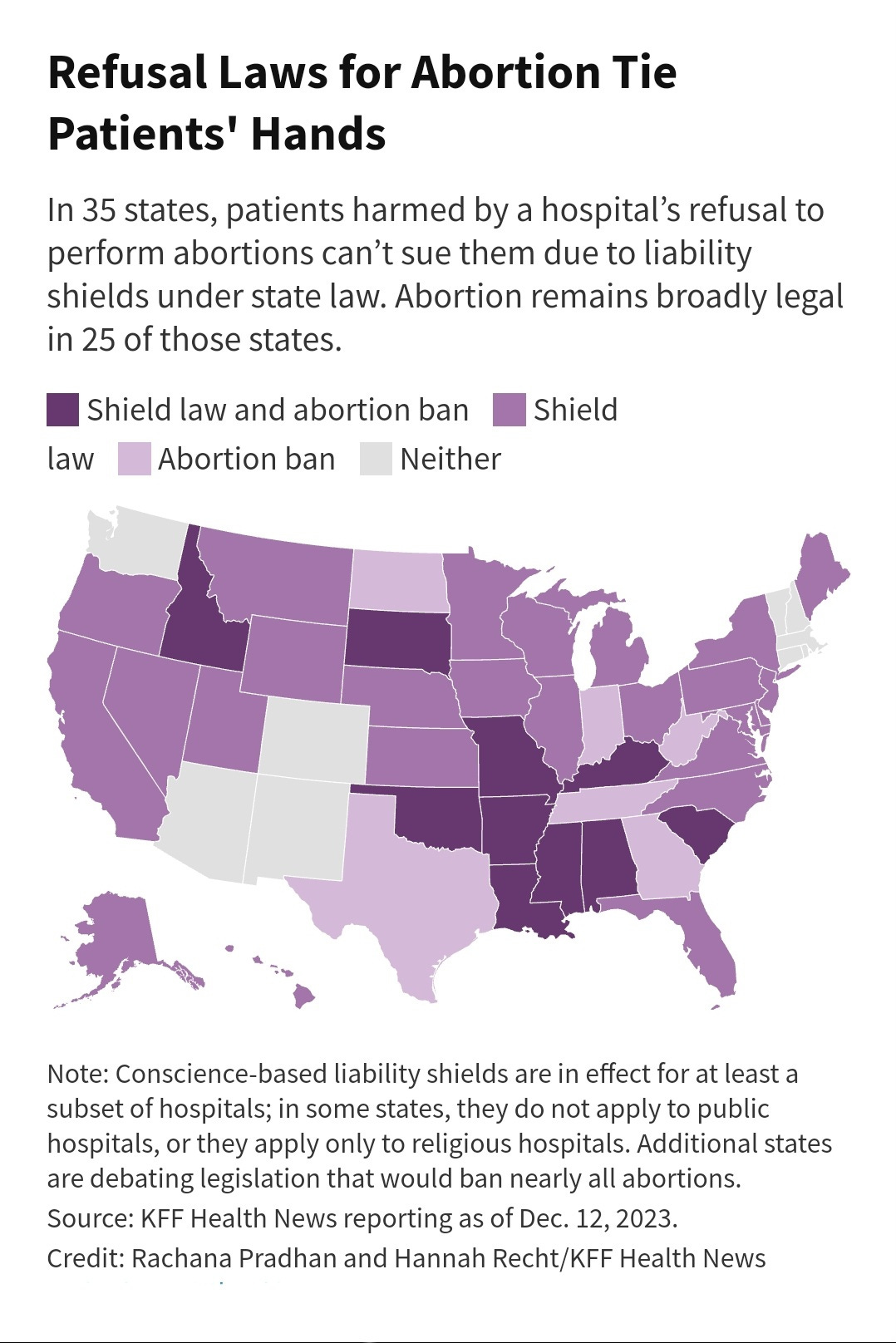
Unfortunately, patients have little recourse or protections. “[I]n most of the country, state laws shield at least some hospitals from lawsuits for not performing procedures they object to on religious grounds, leaving little recourse for patients who were harmed because care was withheld. Thirty-five states prevent patients from suing hospitals for not providing abortions… About half of those laws don’t include exceptions for emergencies, ectopic pregnancies, or miscarriages.”53
Health Care Denied - American Civil Liberties Union. 2016, https://www.aclu.org/sites/default/files/field_document/healthcaredenied.pdf.
Health Care Denied - American Civil Liberties Union. 2016, https://www.aclu.org/sites/default/files/field_document/healthcaredenied.pdf.
Stewart, K. (2022, February 25). Why was a Catholic hospital willing to gamble with my life?. The New York Times. https://www.nytimes.com/2022/02/25/opinion/sunday/roe-dobbs-miscarriage-abortion.html
Recht, H., & Pradhan, R. (2024, March 1). The powerful constraints on medical care in Catholic Hospitals Across America. KFF Health News. https://kffhealthnews.org/news/article/catholic-hospitals-affiliates-ethical-religious-directives-reproductive-care/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
United States Conference Of Catholic Bishops. Ethical and Religious Directives for Catholic Health Care Services. https://www.usccb.org/about/doctrine/ethical-and-religious-directives/upload/ethical-religious-directives-catholic-health-service-sixth-edition-2016-06.pdf.
Health Care Denied - American Civil Liberties Union. 2016, https://www.aclu.org/sites/default/files/field_document/healthcaredenied.pdf.
O’Neill, E. (2022, August 5). A pregnant mom was “writhing in pain,” but a Catholic Hospital refused to intervene. KUOW. https://www.kuow.org/stories/a-pregnant-mom-was-writhing-in-pain-but-a-catholic-hospital-refused-to-intervene
O’Neill, E. (2022, August 5). A pregnant mom was “writhing in pain,” but a Catholic Hospital refused to intervene. KUOW. https://www.kuow.org/stories/a-pregnant-mom-was-writhing-in-pain-but-a-catholic-hospital-refused-to-intervene
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Redden, M. (2016, February 18). Abortion ban linked to dangerous miscarriages at Catholic hospital, report claims. The Guardian. https://www.theguardian.com/us-news/2016/feb/18/michigan-catholic-hospital-women-miscarriage-abortion-mercy-health-partners
Zieglera, M. (2021, August 9). Abortion and the law of innocence. Illinois Law Review. https://illinoislawreview.org/print/vol-2021-no-3/abortion-and-the-law-of-innocence/#:~:text=In%20this%20hierarchy%2C%20fetal%20life,which%20to%20be%20held%20accountable
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
U.S. Department of Health and Human Services. (n.d.). Disseminated intravascular coagulation (DIC). National Heart Lung and Blood Institute. https://www.nhlbi.nih.gov/health/disseminated-intravascular-coagulation
U.S. Department of Health and Human Services. (n.d.). Disseminated intravascular coagulation (DIC). National Heart Lung and Blood Institute. https://www.nhlbi.nih.gov/health/disseminated-intravascular-coagulation
U.S. Department of Health and Human Services. (n.d.). Disseminated intravascular coagulation (DIC). National Heart Lung and Blood Institute. https://www.nhlbi.nih.gov/health/disseminated-intravascular-coagulation
Septic shock. NHS inform. https://www.nhsinform.scot/illnesses-and-conditions/blood-and-lymph/septic-shock/#:~:text=Left%20untreated%2C%20toxins%20produced%20by,as%20the%20brain%20and%20liver.
Septic shock. NHS inform. https://www.nhsinform.scot/illnesses-and-conditions/blood-and-lymph/septic-shock/#:~:text=Left%20untreated%2C%20toxins%20produced%20by,as%20the%20brain%20and%20liver.
Septic shock. NHS inform. https://www.nhsinform.scot/illnesses-and-conditions/blood-and-lymph/septic-shock/#:~:text=Left%20untreated%2C%20toxins%20produced%20by,as%20the%20brain%20and%20liver.
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Investigation of Incident 50278 from time of patient’s self referral to hospital on the 21st of October 2012 to the patient’s death on the 28th of October, 2012.
https://www.hse.ie/eng/services/news/nimtreport50278.pdf
Investigation of Incident 50278 from time of patient’s self referral to hospital on the 21st of October 2012 to the patient’s death on the 28th of October, 2012.
https://www.hse.ie/eng/services/news/nimtreport50278.pdf
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Health Care Denied - American Civil Liberties Union. 2016, https://www.aclu.org/sites/default/files/field_document/healthcaredenied.pdf.
Health Care Denied - American Civil Liberties Union. 2016, https://www.aclu.org/sites/default/files/field_document/healthcaredenied.pdf.
Health Care Denied - American Civil Liberties Union. 2016, https://www.aclu.org/sites/default/files/field_document/healthcaredenied.pdf.
Health Care Denied - American Civil Liberties Union. 2016, https://www.aclu.org/sites/default/files/field_document/healthcaredenied.pdf.
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Pradhan, R., & Recht, H. (2024, February 17). “we can’t do anything”: How catholic hospitals constrain medical care in America. USA Today. https://www.usatoday.com/story/news/nation/2024/02/17/catholic-hospitals-leave-patients-at-the-mercy-of-religious-directives/72634772007/
Redden, M. (2016, February 18). Abortion ban linked to dangerous miscarriages at Catholic hospital, report claims. The Guardian. https://www.theguardian.com/us-news/2016/feb/18/michigan-catholic-hospital-women-miscarriage-abortion-mercy-health-partners
Redden, M. (2016, February 18). Abortion ban linked to dangerous miscarriages at Catholic hospital, report claims. The Guardian. https://www.theguardian.com/us-news/2016/feb/18/michigan-catholic-hospital-women-miscarriage-abortion-mercy-health-partners
Redden, M. (2016, February 18). Abortion ban linked to dangerous miscarriages at Catholic hospital, report claims. The Guardian. https://www.theguardian.com/us-news/2016/feb/18/michigan-catholic-hospital-women-miscarriage-abortion-mercy-health-partners
Redden, M. (2016, February 18). Abortion ban linked to dangerous miscarriages at Catholic hospital, report claims. The Guardian. https://www.theguardian.com/us-news/2016/feb/18/michigan-catholic-hospital-women-miscarriage-abortion-mercy-health-partners
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Freedman, L. R., Landy, U., & Steinauer, J. (2008, October). When there’s A heartbeat: Miscarriage management in Catholic-owned hospitals. American journal of public health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636458/
Pradhan, R., & Recht, H. (2024, February 17). “we can’t do anything”: How catholic hospitals constrain medical care in America. USA Today. https://www.usatoday.com/story/news/nation/2024/02/17/catholic-hospitals-leave-patients-at-the-mercy-of-religious-directives/72634772007/
Pradhan, R., & Recht, H. (2024, February 17). “we can’t do anything”: How catholic hospitals constrain medical care in America. USA Today. https://www.usatoday.com/story/news/nation/2024/02/17/catholic-hospitals-leave-patients-at-the-mercy-of-religious-directives/72634772007/
Bearing faith. Bearing Faith | Law, Rights, and Religion Project. (2018, January). https://lawrightsreligion.law.columbia.edu/bearingfaith
Bearing faith. Bearing Faith | Law, Rights, and Religion Project. (2018, January). https://lawrightsreligion.law.columbia.edu/bearingfaith
Bearing faith. Bearing Faith | Law, Rights, and Religion Project. (2018, January). https://lawrightsreligion.law.columbia.edu/bearingfaith
Russell-Kraft, S. (2021, May 11). How religious health care hurts women of color. The New Republic. https://newrepublic.com/article/146657/religious-health-care-hurts-women-color
Russell-Kraft, S. (2021, May 11). How religious health care hurts women of color. The New Republic. https://newrepublic.com/article/146657/religious-health-care-hurts-women-color
Russell-Kraft, S. (2021, May 11). How religious health care hurts women of color. The New Republic. https://newrepublic.com/article/146657/religious-health-care-hurts-women-color
Russell-Kraft, S. (2021, May 11). How religious health care hurts women of color. The New Republic. https://newrepublic.com/article/146657/religious-health-care-hurts-women-color
Pradhan, R., & Recht, H. (2024, February 17). “we can’t do anything”: How catholic hospitals constrain medical care in America. USA Today. https://www.usatoday.com/story/news/nation/2024/02/17/catholic-hospitals-leave-patients-at-the-mercy-of-religious-directives/72634772007/